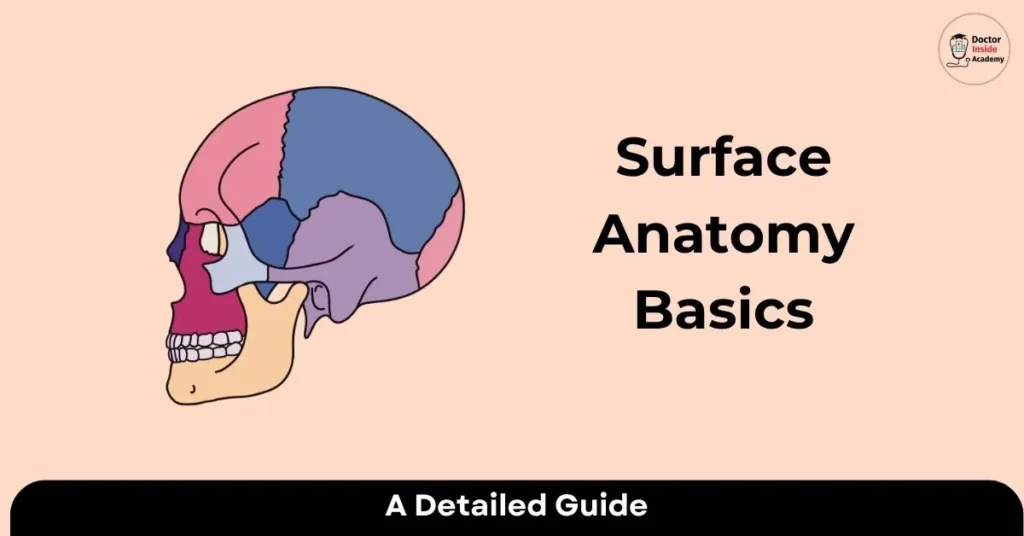
Surface anatomy (also called superficial anatomy) is the study of external body features and landmarks that can be observed or felt (palpated) without dissection. It is a branch of gross anatomy that links surface markings to the deeper structures, such as bones, muscles, and organs, hidden beneath the skin.
What is Gross Anatomy?
Like other scientific fields, anatomy includes areas of expertise. Gross anatomy examines the body’s bigger structures, such as internal organs and external features, that may be seen without the need for magnification. Because “large” means “macro” in Greek, gross anatomy is also known as macroscopic anatomy.
The study of an animal’s exterior characteristics is known as surface anatomy, often referred to as superficial anatomy or visible anatomy. This is known as topography in birds. Surface anatomy is the study of anatomical characteristics that may be observed without dissection. Together with endoscopic and radiological anatomy, it is therefore a subfield of gross anatomy.
The science of surface anatomy is descriptive. Specifically, in the context of human surface anatomy, they are the shape and dimensions of the human body as well as the surface landmarks that, both in motion and in a stationary position, correlate to deeper structures that are concealed from view.
It is crucial to find and recognize anatomic structures before learning about the interior gross anatomy.
It aids in identifying the organ, structure, or area impacted by the illness.
There are Four Methods for Analyzing Surface Anatomy:
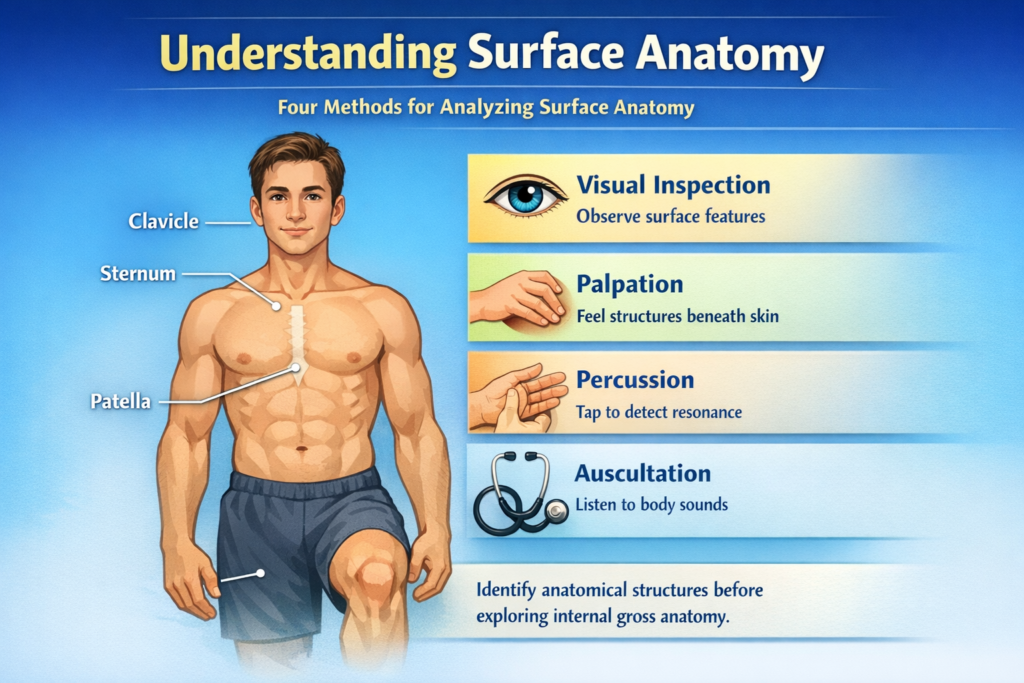
- Visual inspection: Examine the surface features’ marks and structure firsthand.
- Palpation: Experiencing with solid pressure or perceiving via the sense of(touch), accurately discover and recognize anatomical structures beneath the skin.
- Use Percussion: to find resonance vibrations by tapping firmly on particular body locations.
- Auscultation: hear the noises that organs make
Practical Foundations of Surface Anatomy
The instruments of surface anatomy are the fingers. The body’s structures with the most proprioceptors, aside from the face and tongue with the mouth, are the fingers, which have about 300 receptors per square centimeter of skin.
The index finger is the most crucial digit for recognizing surface anatomy because of its high mobility.
The examiner tries to feel, inspect, and identify the underlying tissue by exerting pressure with the fingertips.
The kind of tissue may be directly inferred from the amount of pressure applied and the structure’s resistance to the pressure.
- Hard: Structures (bone or horn) that the examiner’s hand cannot bend.
- Firm and Elastic: Structures (such as tendons and ligaments) that can withstand pressure and gently bounce back without deforming.
- Firm: Non-elastic structures that readily yield to pressure (e.g., hypertonic muscles, tumors).
- Soft: Tissue that is easily distorted, such as muscles or fatty tissue.
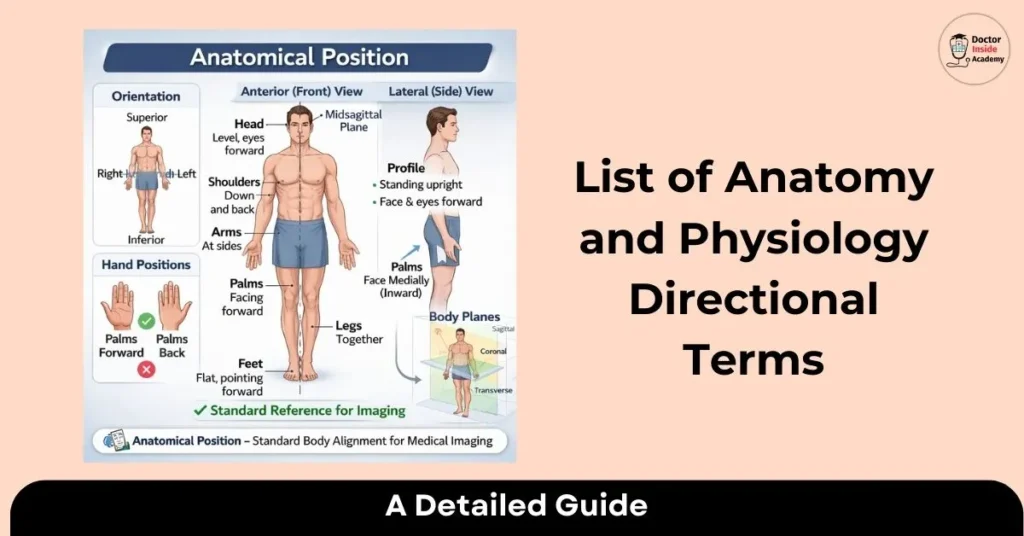
Standard Anatomical References
All surface landmarks, standing upright, arms at the sides, palms facing forward, and eyes looking toward the horizon, are specified in relation to the anatomical posture to maintain uniformity.
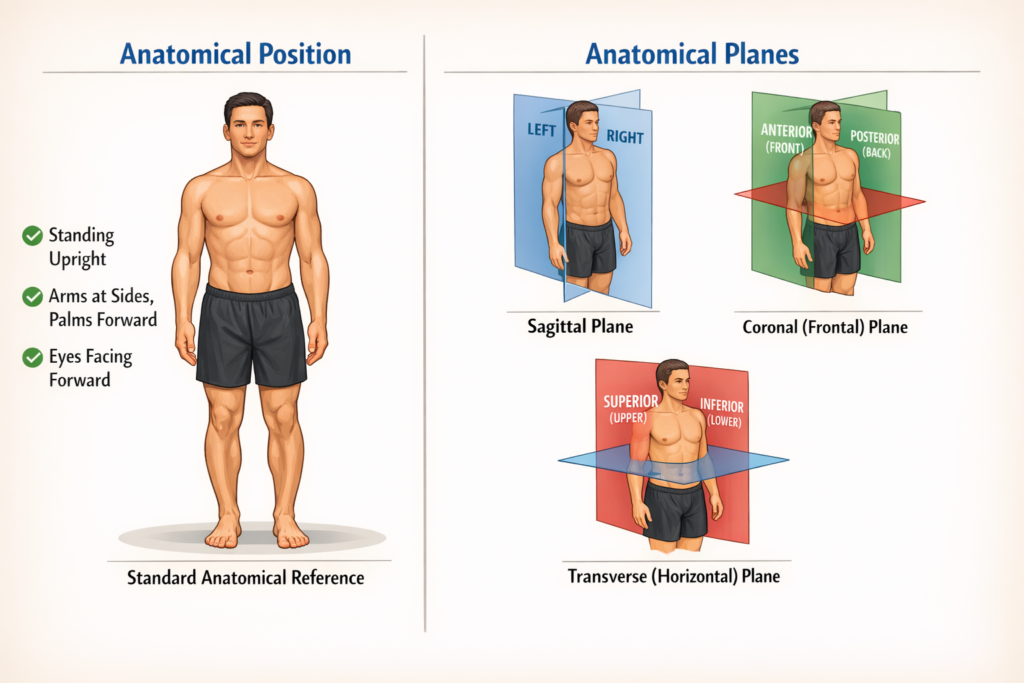
Anatomical planes are another conceptual division of the body:
- Sagittal: Separates the left and right sides of the body.
- Coronal (Frontal): Separates the body into anterior (front) and posterior (rear) halves.
- Transverse (Horizontal): Separates the upper (superior) and lower (inferior) halves of the body.
Surface Anatomy of the Head
Clinical mapping is based on the bony markers that characterize the head’s surface anatomy. The supraorbital ridges above the eyes and the frontal bone that forms the forehead are important characteristics. The mastoid process, the solid hump behind the ear, serves as a crucial location for muscle attachment and direction during physical examinations, while the zygomatic arch forms the prominent cheekbone on the sides of the face.
Moving down to the lower face, the mandible offers a number of perceptible markers that are crucial for surgical and dental operations. The angle of the mandible indicates the posterior border of the jaw, whilst the mental protuberance creates the chin at the midline.
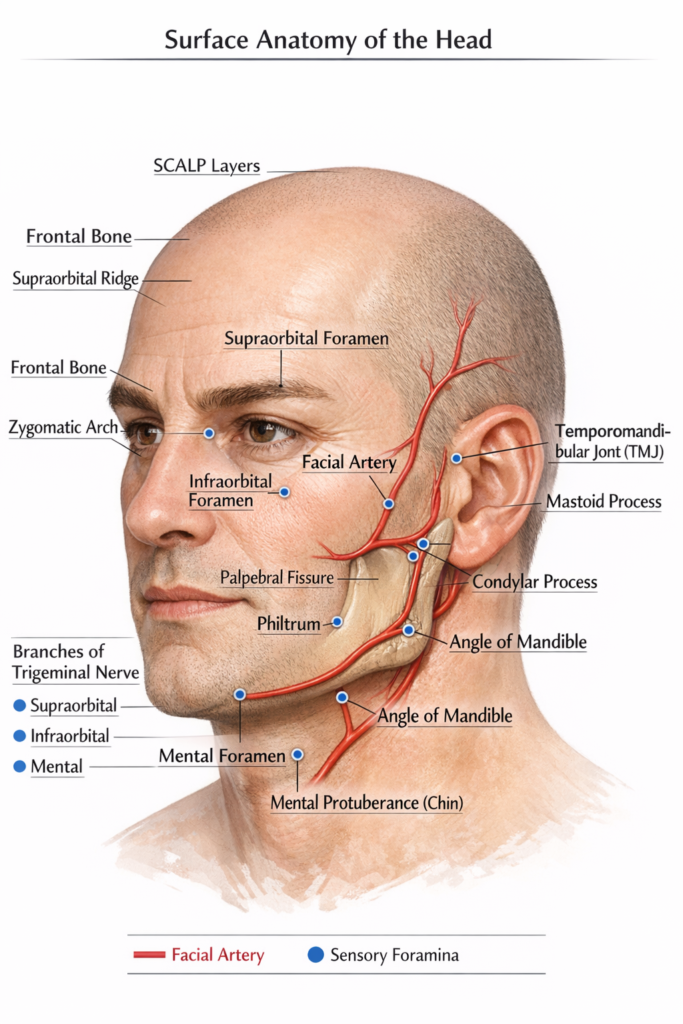
The temporomandibular joint, a common site of clinical evaluation for jaw dysfunction, can be found by touching the condylar process immediately anterior to the ear while expanding the mouth.
The SCALP, a five-layered structure covering the neurocranium, dominates the soft tissue of the skull. Loose areolar tissue, the fourth layer, is clinically relevant as the “danger zone” because it facilitates the quick spread of infection or fluid. The palpebral fissures of the eyes and the philtrum above the top lip are additional visible soft tissue indicators that are utilized to evaluate facial symmetry and possible nerve injury.
Lastly, important arteries and nerves may be located non-invasively thanks to neurovascular landmarks. The facial artery is felt along the bottom line of the jaw, and the superficial temporal artery can be felt for a pulse directly in front of the ear. Additionally, three vertically aligned foramina, the supraorbital, infraorbital, and mental, mark the exit points for branches of the trigeminal nerve, serving as precise targets for administering local anesthesia or testing facial sensation.
Surface Anatomy of Neck
The sternocleidomastoid muscle, which is the most noticeable surface landmark when the head is twisted, mainly divides the neck into anterior and posterior triangles. The thyroid cartilage, sometimes referred to as the “Adam’s apple,” and the hyoid bone, which moves during swallowing, are located in the anterior triangle. Just below this lies the cricoid cartilage and the thyroid gland, which are essential landmarks for emergency procedures like a cricothyroidotomy or for palpating the trachea’s alignment.
In order to evaluate circulatory health and provide therapy, neurovascular landmarks in the neck are essential. At the level of the upper border of the thyroid cartilage, the carotid pulse is easily palpable in the groove between the trachea and the sternocleidomastoid muscle.
Furthermore, the external jugular vein frequently crosses the sternocleidomastoid muscle diagonally, acting as a location for peripheral venous access in an emergency and a visual sign of venous pressure.
The trapezius muscle and the vertebral column’s bony markers define the posterior surface anatomy of the neck. The most prominent bony protrusion at the base of the neck is the vertebra prominens, or the spinous process of the C7 vertebra, which is reached by the nuchal groove running along the midline. During physical exams, this point is the main point of reference for counting vertebrae and locating the change from the cervical to the thoracic spine.
Surface Anatomy of Trunk
The midline and thoracic cage, which act as reference points for internal organs, largely determine the surface anatomy of the trunk. A perceptible horizontal ridge on the breastbone that indicates the level of the second rib, the sternal angle (also known as the Angle of Louis), is crucial for quantifying intercostal gaps during lung and heart tests.
The costal margins, or the V-shaped bottom border of the ribs, delineate the upper limit of the abdomen as well as the location of the stomach and liver, while the xiphoid process indicates the lower end of the sternum.
The umbilicus, or belly button, serves as the primary marker for segmenting the abdominal region into four quadrants or nine areas to identify abdominal discomfort.
For spinal surgeries, the L4 vertebra can be found by feeling the iliac crests, or hip bones, on the lower trunk. Important surface indicators for locating muscle borders and possible hernia sites include the inguinal ligaments, which form the crease between the torso and the thighs, and the linea alba, a vertical groove that runs down the middle of the belly.
Surface Anatomy of Shoulder and Upper Limbs
The acromion, clavicle, and scapular spine are the three major bony characteristics that identify the shoulder. When injecting intramuscularly into the deltoid muscle, the acromion, the high point of the shoulder, is a crucial marker. The coracoid process of the scapula is palpable at the “deltopectoral triangle,” which is a crucial point of reference for neurovascular systems such as the axillary artery, and the larger tubercle of the humerus can be felt on the lateral side just below this.
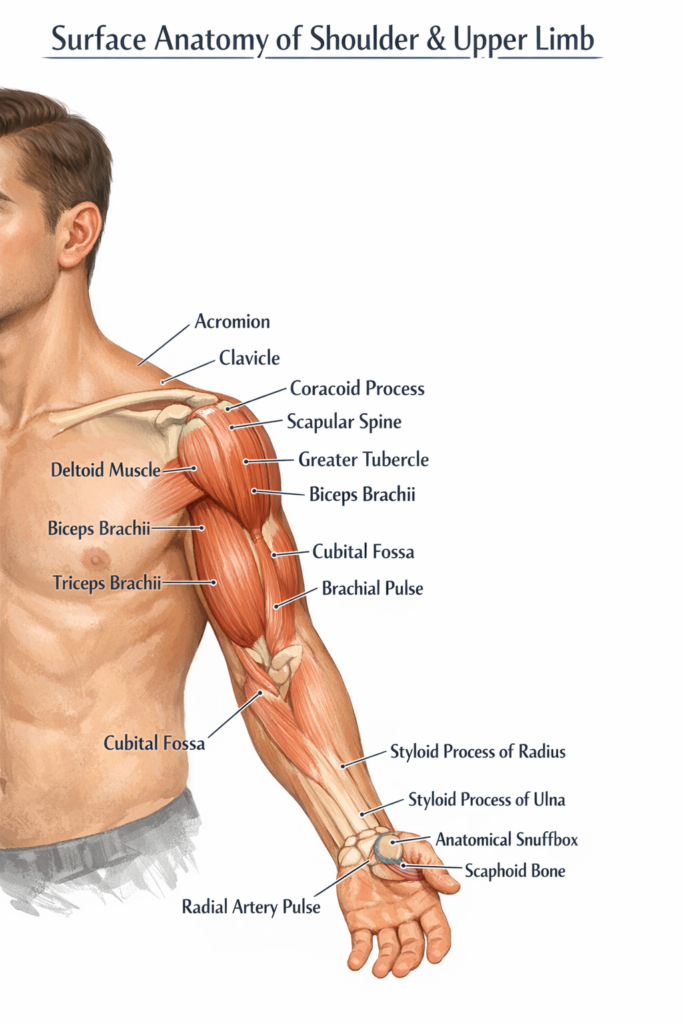
The cubital fossa, or pit of the elbow, is a key location for taking blood and feeling the brachial pulse. The biceps brachii and triceps brachii in the arm and hand form the visible features of the upper arm. The ulna and radius styloid processes are readily palpable on either side of the wrist. The anatomical snuffbox, a little indentation at the base of the thumb where the radial pulse may be identified, and the scaphoid bone can be evaluated for fractures, is a particularly well-known landmark.
Surface Anatomy of the Buttocks and Lower Limbs
The big gluteus maximus muscle, which gives the buttocks their rounded shape, is what defines it. The iliac crest, which is the top border of the hip bone and is felt around the waist, is the most important surface feature in this situation.
The greater trochanter of the femur is a firm protrusion on the lateral side of the hip, whereas the ischial tuberosity (sometimes known as the “sitting bone”) is located just below the center of the buttock. Intramuscular injections are often administered in the upper outer quadrant of the buttock, which is clinically divided into four quadrants, to prevent injury to the large sciatic nerve that passes deep into the core.
The most noticeable feature in the lower extremities is the patella, or kneecap, which is located inside the tendon of the strong quadriceps femoris muscle. The popliteal fossa, a diamond-shaped depression behind the knee, is where the popliteal pulse can be felt deep into the soft tissue.
Moving down to the ankle, the medial and lateral malleoli are the bony “bumps” on either side of the joint. On the foot, the dorsalis pedis artery can be felt on the upper surface (dorsum) between the first and second metatarsals, serving as a vital check for peripheral circulation.
Last Words
Understanding surface anatomy is crucial for bridging the gap between internal diagnosis and outward observation. The location of underlying organs, muscles, and neurovascular routes may be precisely mapped utilizing palpable bone markers such as the iliac crest, sternal angle, and acromion. These surface markers offer the “GPS coordinates” required for safe and efficient clinical treatment, whether you are detecting a pulse in the carotid artery or identifying injection sites in the gluteal or deltoid areas.
In the end, these physical indicators, from the malleoli of the ankles to the foramina of the face, allow for a quick, non-invasive evaluation of a patient’s health. Precision in everything from basic physical examinations to urgent surgical treatments is ensured by regular practice in detecting these features through touch and scrutiny.